Quiz-summary
0 of 2 questions completed
Questions:
- 1
- 2
Information
You have already completed the quiz before. Hence you can not start it again.
Quiz is loading...
You have to finish following quiz, to start this quiz:
Results
0 of 2 questions answered correctly
Your time:
Time has elapsed
You have reached 0 of 0 points, (0)
| Average score |
|
| Your score |
|
Categories
- Uterus 0%
- 1
- 2
- Answered
- Review
-
Question 1 of 2
1. Question
HPI: 33 year old G2P1
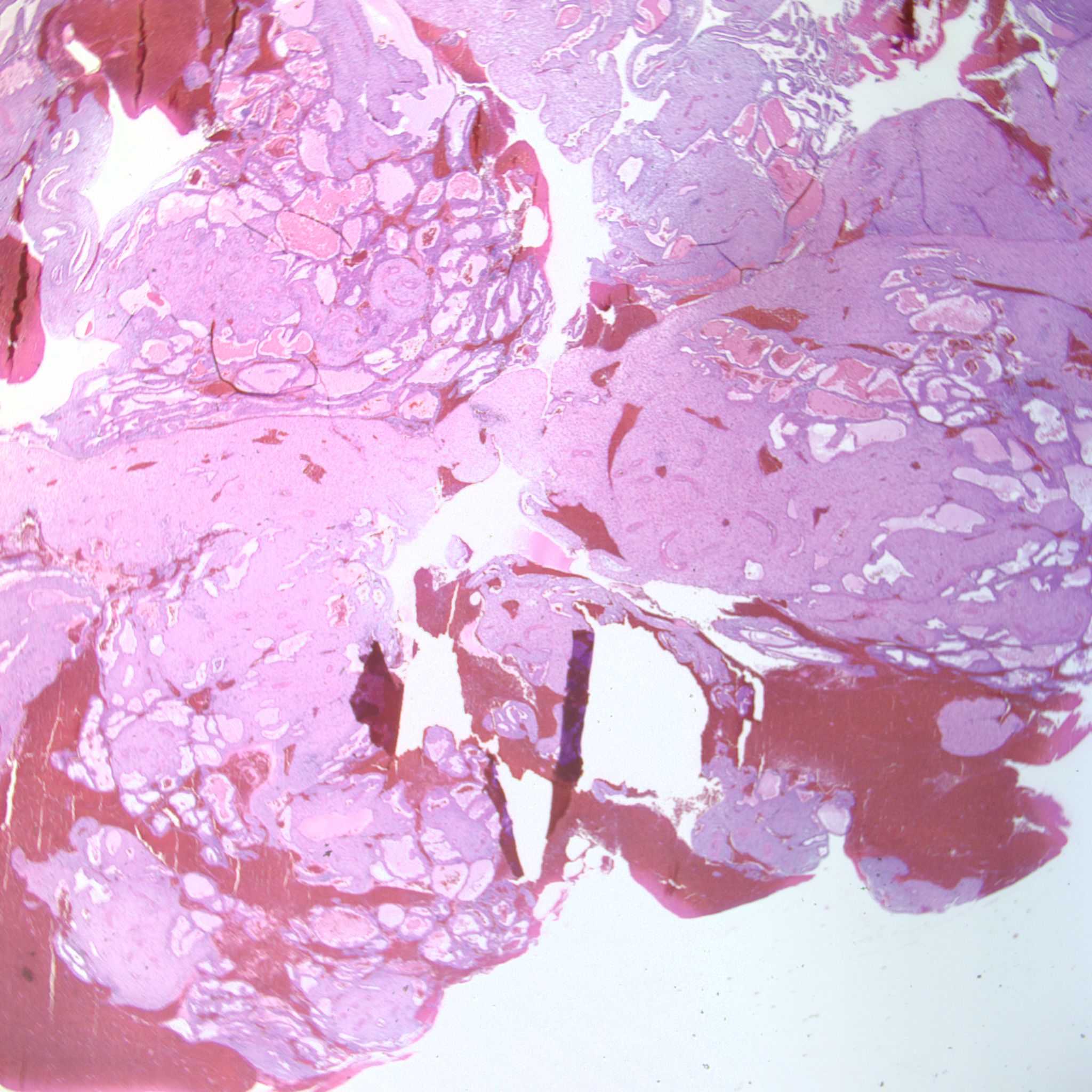
Gross: Received are multiple fragments of red-brown soft tissue (23.0 x 14.0 x 4.4cm) in maximum dimensions. Chorionic villi but no fetal tissue are identified. Non-clot areas were entirely submitted.Images:

What is your diagnosis?
Correct
Diagnosis: Complete Hydatidiform Mole

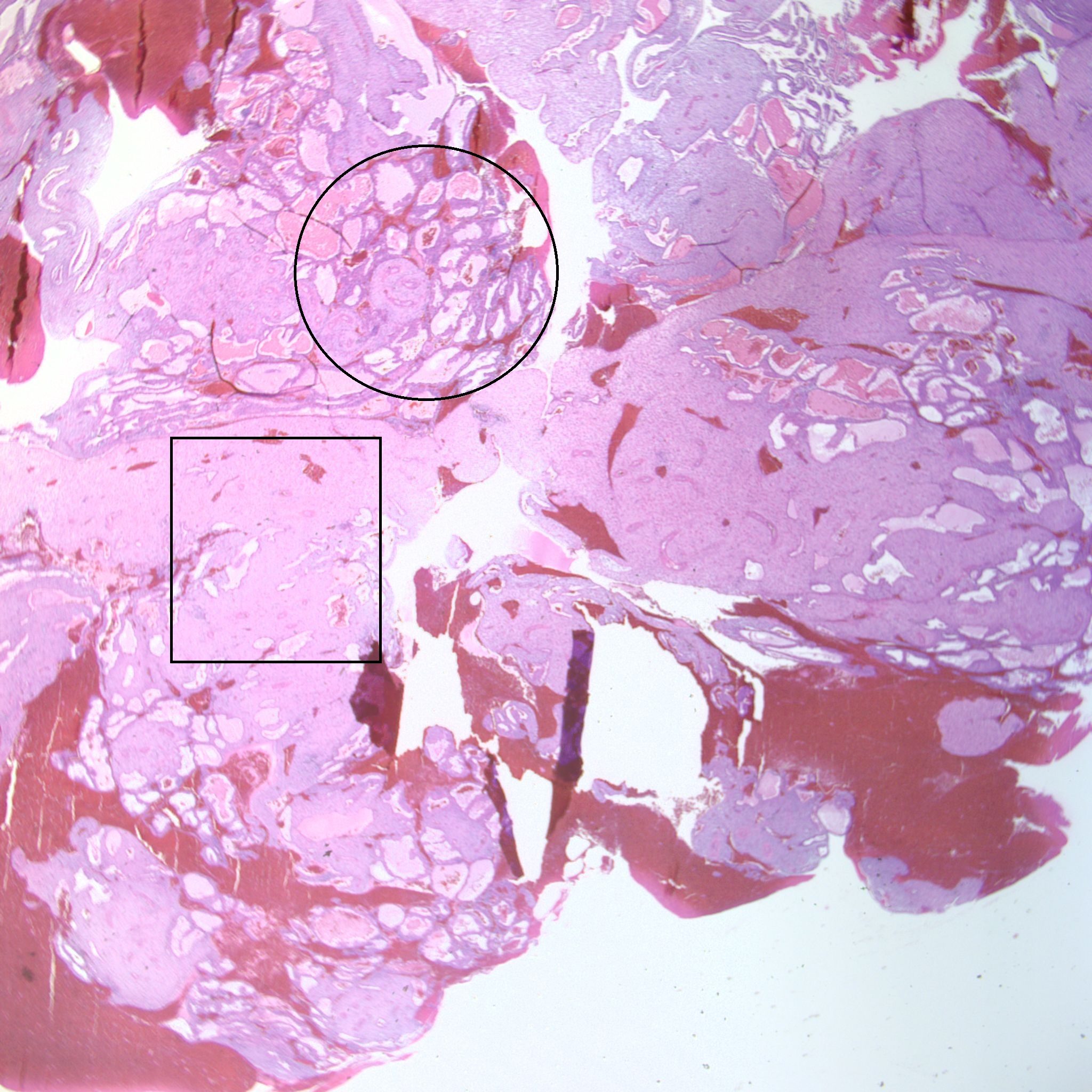
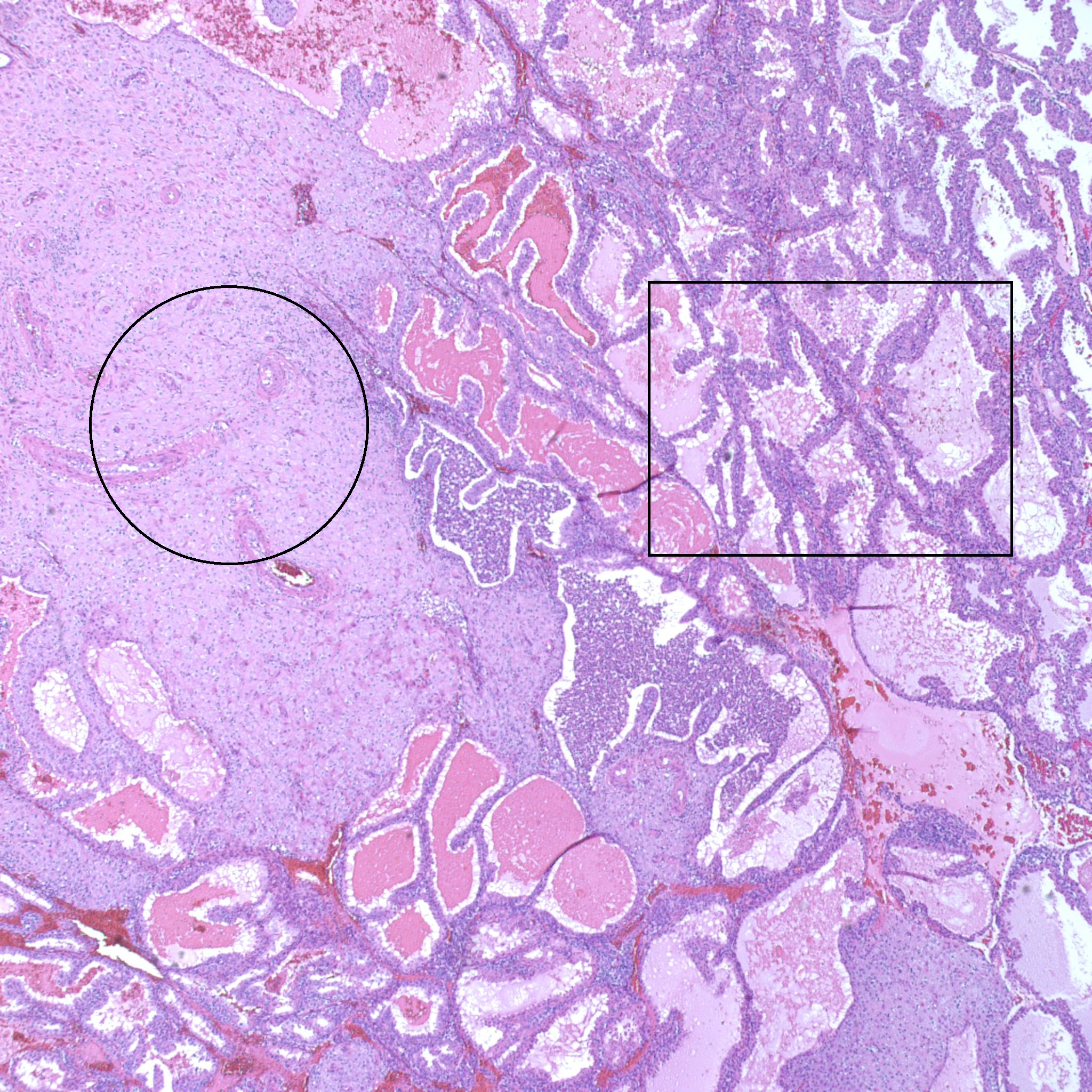
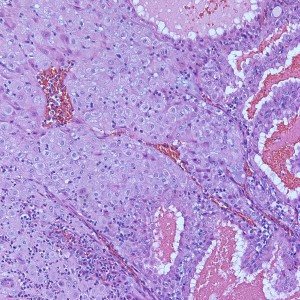
At low power, the majority of the specimen consists of decidua (square) and gestational-type endometrium (circle).
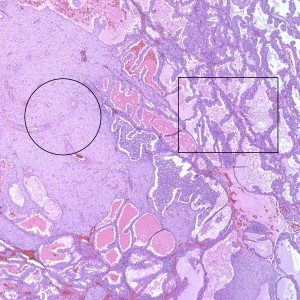
At medium power, we also see decidua (circle) and gestational endometrium (rectangle)
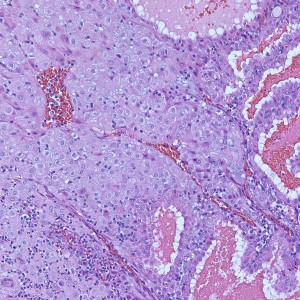
Higher power of unremarkable decidua with gestational-type endometrium
Gestational-type Endometrium
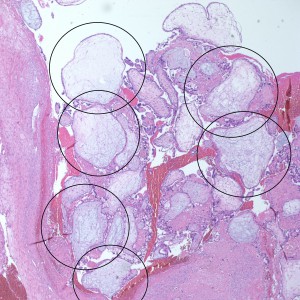
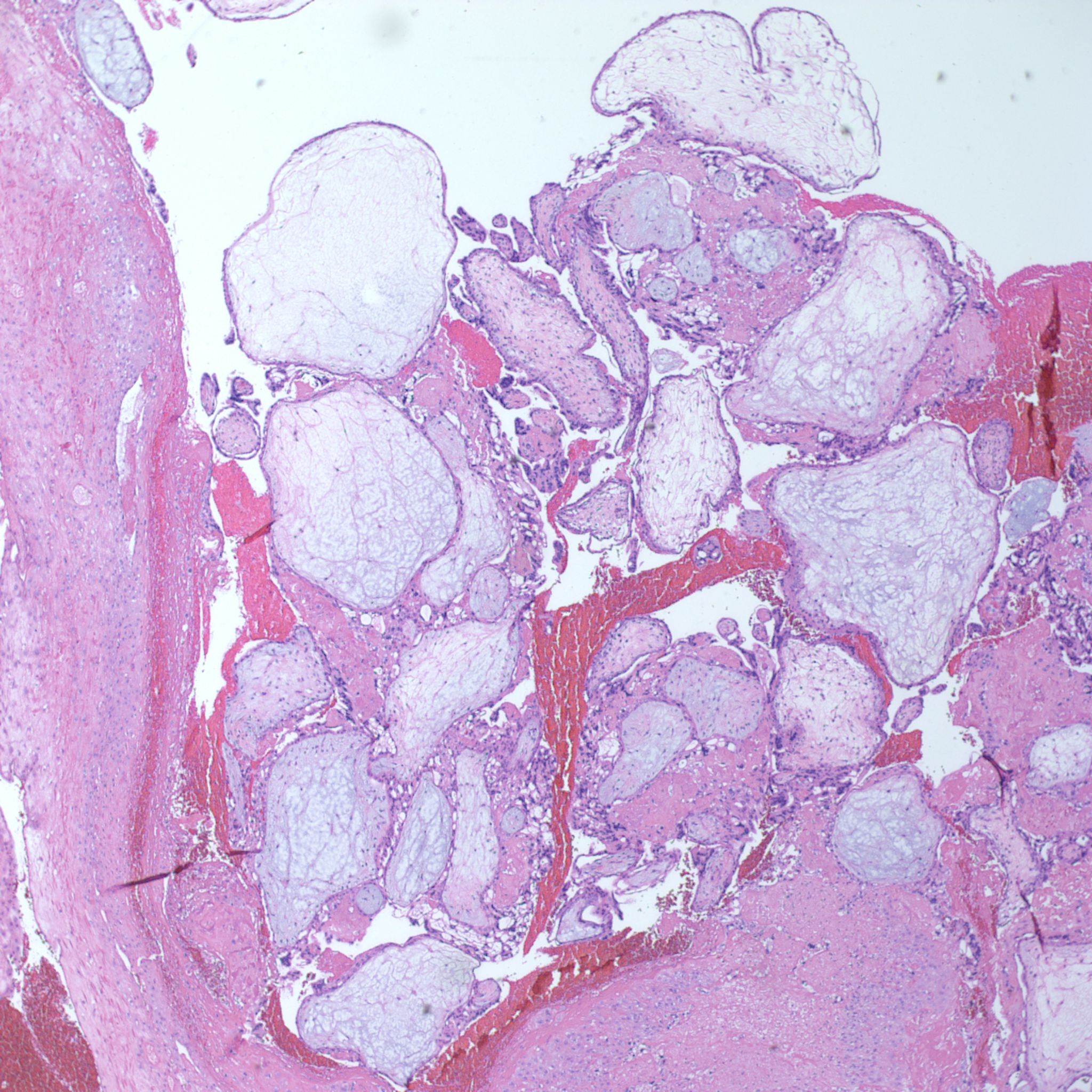
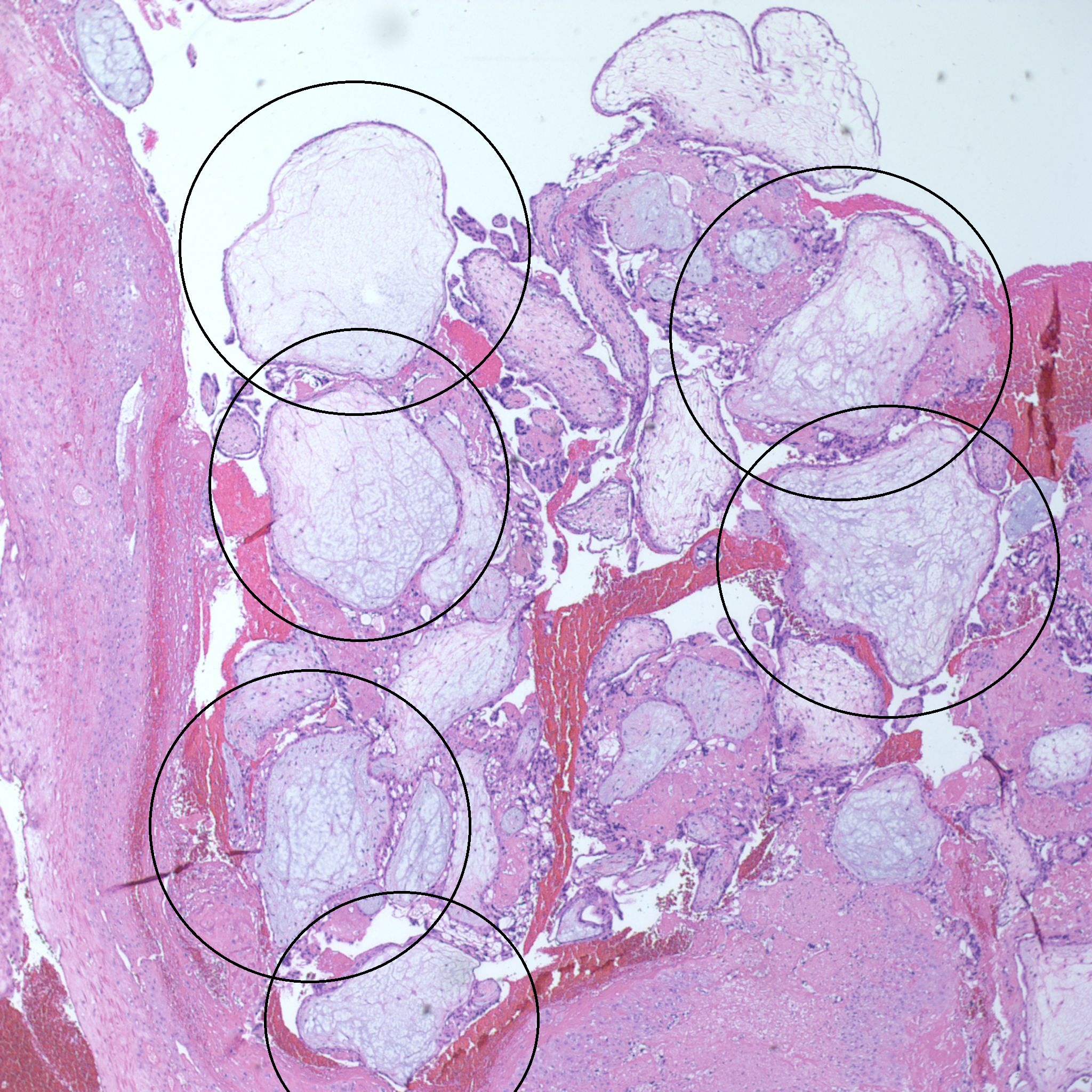
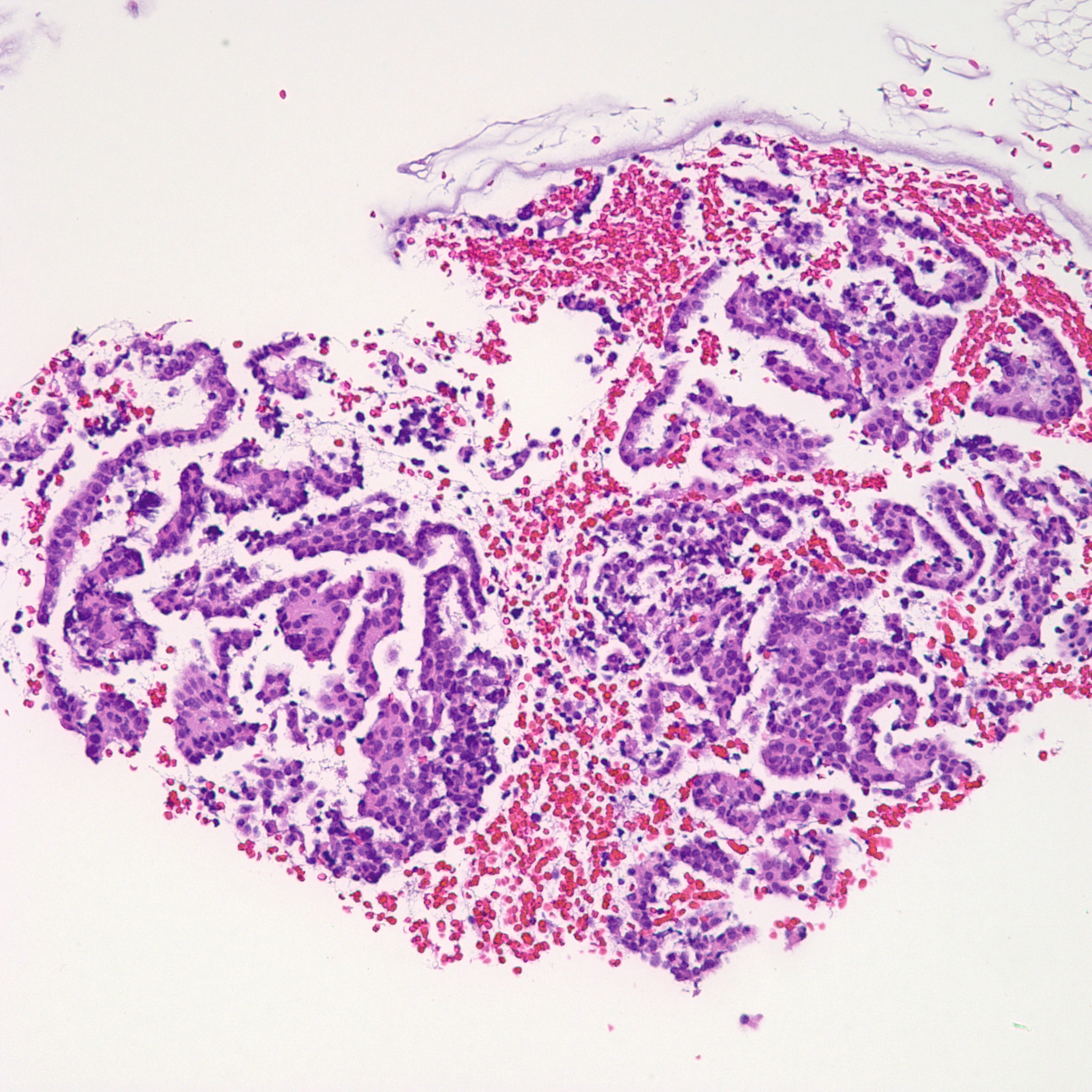
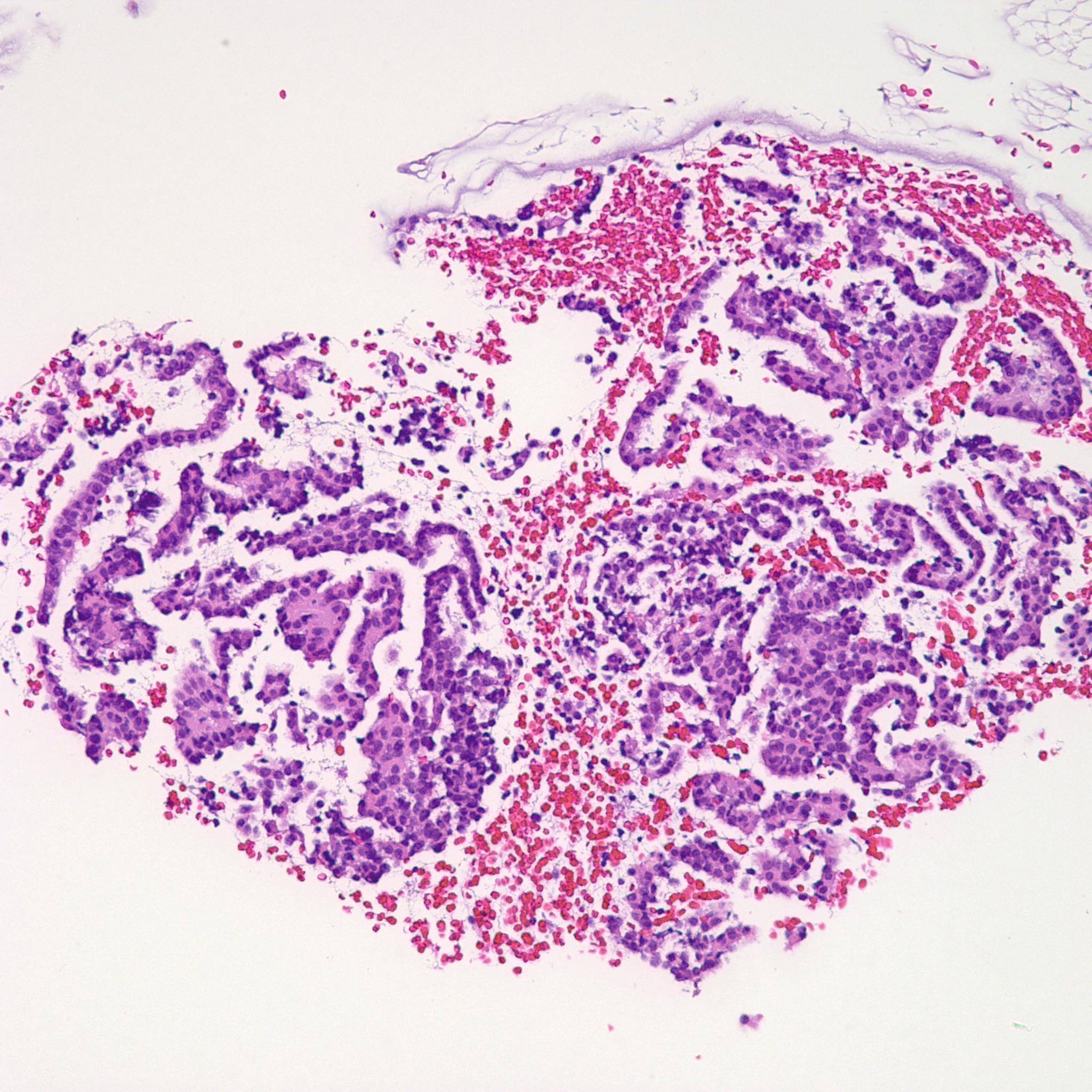
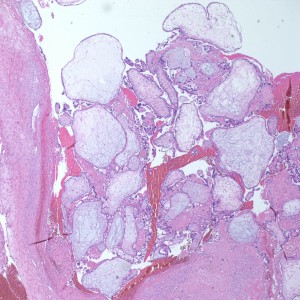
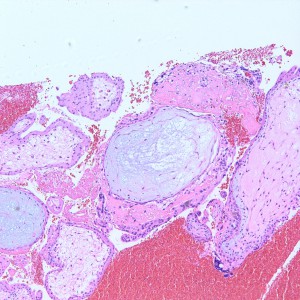
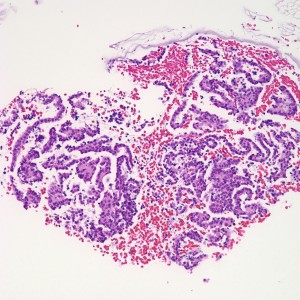
At low power we see throughout the specimen that numerous enlarged hydropic chorionic villi are present (circles).
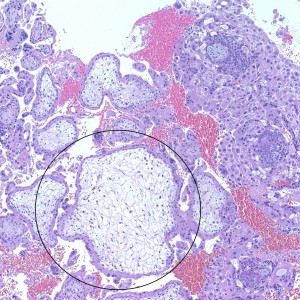
As we can see, enlarged and hydropic chorionic villi are not especially difficult to find (circle). None of these villi however demonstrate trophoblastic inclusions. There are rare interspersed small chorionic villi (top left) however they are generally rare.
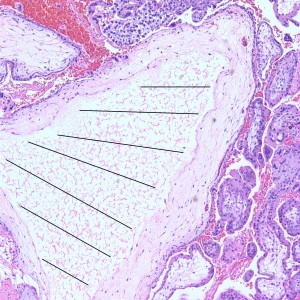
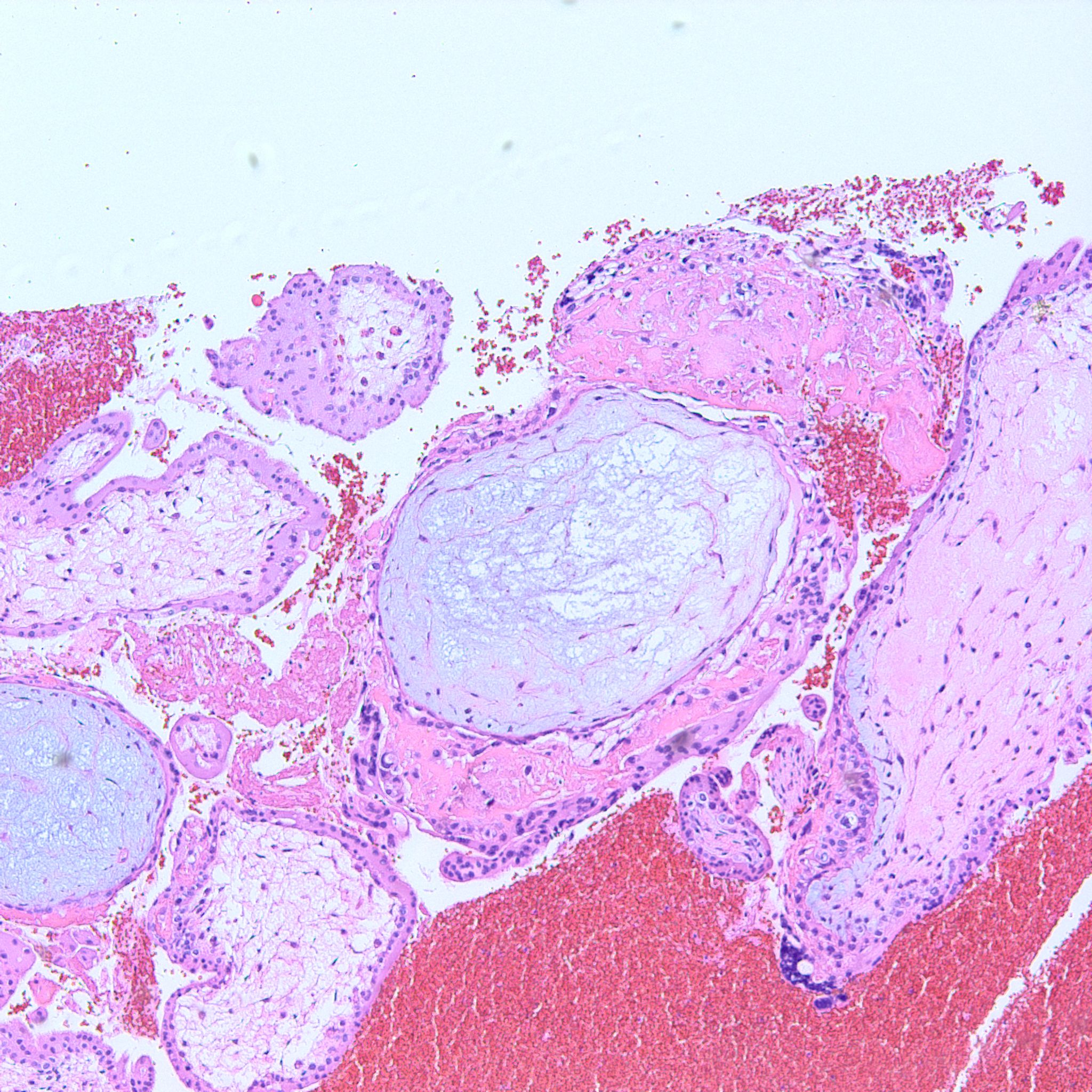
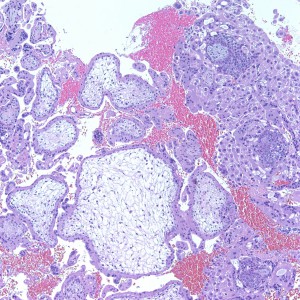
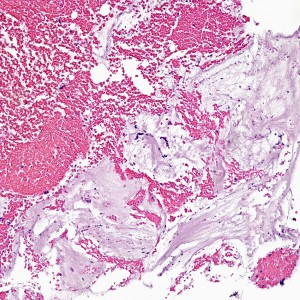
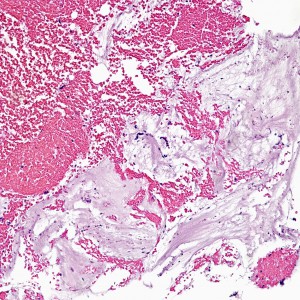
Some villi are so large and hydropic that a few have actually developed central cisterns, spaces within the center of the villi (space highlighted by horizontal lines).
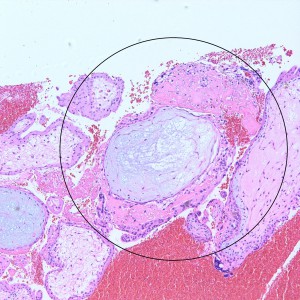
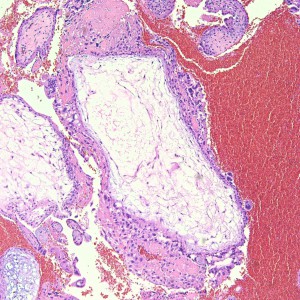
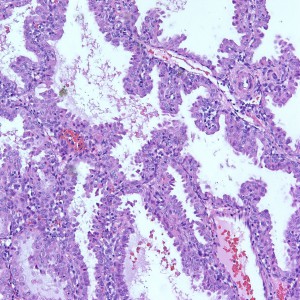
Hydropic villi with some circumferential trophoblastic proliferation.

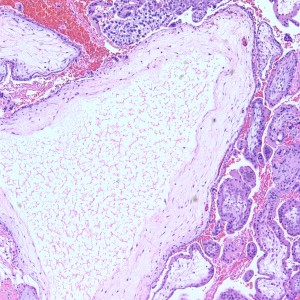
This large hydropic villus with central cistern also demonstrates an important finding: the loss of polarity of the surrounding trophoblasts with circumferential proliferation of variably atypical trophoblastic cells (arrows).
Case Discussion:Complete hydatidiform moles are a form of gestational trophoblastic disease (GTD). Gestational trophoblastic diseases are diseases of abnormal trophoblastic proliferations.WHO categories: (GTD)- Molar Lesions
- Hydatidiform mole
- Complete
- Partial
- Invasive Mole
- Hydatidiform mole
- Non-Molar Lesions
- Choriocarcinoma
- Placental Site Trophoblastic Tumor (PSTT)
- Epithelioid trophoblastic tumor
- Trophoblastic lesions (Non-Molar and Non-Neoplastic Lesions)
- Exaggerated placental site
- Placental site nodule
Complete moles that occurred typically in the second trimester (after 13 weeks gestation) are known as “classic” complete moles, with florid and distinct clinical and histopathology. In the classic mole, patients present in the second trimester with uterine enlargement greater than expected for gestational age, quite often with abortion with abnormal bleeding and passage of molar tissue. Ultrasound shows a “snowstorm” picture and there are no observed fetal heart tones. Because of increased ultrasonography earlier in the pregnancy, the “classic” complete molar presentation has become less common and the diagnosis has become more difficult, with a less florid presentation.
As is the case for most GTDz, complete moles typically produce elevated beta-HCG.
Pathogenesis: In most cases, complete moles form from the irregular fertilization and proliferation of an empty maternal egg by a single or two sperm: The karyotype of these lesions is 46XX (diploid) or tetraploid, entirely composed of paternal DNA.
Grossly: The features of a complete hydatidiform mole, in the classic sense, is described as a loose aggregation of vesicles representing a cluster of grapes and fetal tissue often rare or absent.
Histologically, chorionic villi will demonstrate generalized swelling with round to bulbous villi with frequent central cistern formation, with circumferential and multifocal peri-villous trophoblastic proliferation often with significant trophoblastic atypia. As aforementioned, fetal tissue is rare to absent. Trophoblastic inclusions are more characteristic of partial moles and are not a frequent finding in complete moles.
It is important to identify and distinguish between complete and partial mole because complete moles are at higher risk for persistent GTD. Persistent GTD may demonstrate recurrence of the original mole, or there may be the progression of the molar pregnancy into an invasive mole that infiltrates into the uterine myometrium. Rarely, choriocarcinoma can develop from molar pregnancies.
Clinical and Cytogenetic Comparison of Hydatiform Moles Feature Complete Mole Partial Mole Presentation Spontaneous Abortion Missed Abortion Gestation Age 8-18 weeks 8-22 weeks hCG titer Typically elevated Low to Normal Uterine Size Often enlarged for date Often small for date Amount of Tissue Variable, may be increased Variable, may be decreased Karyotype Most commonly 46XX(all paternal) 69XXY or XXX (2:1 paternal to maternal, most often) Persistent GTD 15-20% ~1% Comparison of Pathologic Features of Complete Mole , Partial Mole, and Hydropic Mole Feature Complete Mole Partial Mole Villous Hydrops Generalized and often seen grossly Partial, may be seen grossly Villous Shape Round to bulbous Irregular, scalloped Cisterns Present Present Trophoblastic Inclusions Rare Common Fetal Tissue Rare Common Trophoblast Distribution Circumferential, multifocal (non-polar) Circumferential, multifocal (non-polar) Trophoblast Proliferation Variable, may be marked Focal, minimal Trophoblast Atypia Often present Rare Treatment:
Typically, D&C is performed to initially remove molar tissue. If a molar pregnancy is suspected from the pathological results, HCG levels will be followed until they are undetectable. If HCG fails to decline, methotrexate may also be used to treat the invasive mole. If there is suspicion of a molar pregnancy, the pathology report may provide a comment that biochemical follow-up is recommended.
Incorrect
Diagnosis: Complete Hydatidiform Mole
At low power, the majority of the specimen consists of decidua (square) and gestational-type endometrium (circle).
At medium power, we also see decidua (circle) and gestational endometrium (rectangle)
Higher power of unremarkable decidua with gestational-type endometrium
Gestational-type Endometrium
At low power we see throughout the specimen that numerous enlarged hydropic chorionic villi are present (circles).
As we can see, enlarged and hydropic chorionic villi are not especially difficult to find (circle). None of these villi however demonstrate trophoblastic inclusions. There are rare interspersed small chorionic villi (top left) however they are generally rare.
Some villi are so large and hydropic that a few have actually developed central cisterns, spaces within the center of the villi (space highlighted by horizontal lines).
Hydropic villi with some circumferential trophoblastic proliferation.
This large hydropic villus with central cistern also demonstrates an important finding: the loss of polarity of the surrounding trophoblasts with circumferential proliferation of variably atypical trophoblastic cells (arrows).
Case Discussion:Complete hydatidiform moles are a form of gestational trophoblastic disease (GTD). Gestational trophoblastic diseases are diseases of abnormal trophoblastic proliferations.WHO categories: (GTD)- Molar Lesions
- Hydatidiform mole
- Complete
- Partial
- Invasive Mole
- Hydatidiform mole
- Non-Molar Lesions
- Choriocarcinoma
- Placental Site Trophoblastic Tumor (PSTT)
- Epithelioid trophoblastic tumor
- Trophoblastic lesions (Non-Molar and Non-Neoplastic Lesions)
- Exaggerated placental site
- Placental site nodule
Complete moles that occurred typically in the second trimester (after 13 weeks gestation) are known as “classic” complete moles, with florid and distinct clinical and histopathology. In the classic mole, patients present in the second trimester with uterine enlargement greater than expected for gestational age, quite often with abortion with abnormal bleeding and passage of molar tissue. Ultrasound shows a “snowstorm” picture and there are no observed fetal heart tones. Because of increased ultrasonography earlier in the pregnancy, the “classic” complete molar presentation has become less common and the diagnosis has become more difficult, with a less florid presentation.
As is the case for most GTDz, complete moles typically produce elevated beta-HCG.
Pathogenesis: In most cases, complete moles form from the irregular fertilization and proliferation of an empty maternal egg by a single or two sperm: The karyotype of these lesions is 46XX (diploid) or tetraploid, entirely composed of paternal DNA.
Grossly: The features of a complete hydatidiform mole, in the classic sense, is described as a loose aggregation of vesicles representing a cluster of grapes and fetal tissue often rare or absent.
Histologically, chorionic villi will demonstrate generalized swelling with round to bulbous villi with frequent central cistern formation, with circumferential and multifocal peri-villous trophoblastic proliferation often with significant trophoblastic atypia. As aforementioned, fetal tissue is rare to absent. Trophoblastic inclusions are more characteristic of partial moles and are not a frequent finding in complete moles.
It is important to identify and distinguish between complete and partial mole because complete moles are at higher risk for persistent GTD. Persistent GTD may demonstrate recurrence of the original mole, or there may be the progression of the molar pregnancy into an invasive mole that infiltrates into the uterine myometrium. Rarely, choriocarcinoma can develop from molar pregnancies.
Clinical and Cytogenetic Comparison of Hydatiform Moles Feature Complete Mole Partial Mole Presentation Spontaneous Abortion Missed Abortion Gestation Age 8-18 weeks 8-22 weeks hCG titer Typically elevated Low to Normal Uterine Size Often enlarged for date Often small for date Amount of Tissue Variable, may be increased Variable, may be decreased Karyotype Most commonly 46XX(all paternal) 69XXY or XXX (2:1 paternal to maternal, most often) Persistent GTD 15-20% ~1% Comparison of Pathologic Features of Complete Mole , Partial Mole, and Hydropic Mole Feature Complete Mole Partial Mole Villous Hydrops Generalized and often seen grossly Partial, may be seen grossly Villous Shape Round to bulbous Irregular, scalloped Cisterns Present Present Trophoblastic Inclusions Rare Common Fetal Tissue Rare Common Trophoblast Distribution Circumferential, multifocal (non-polar) Circumferential, multifocal (non-polar) Trophoblast Proliferation Variable, may be marked Focal, minimal Trophoblast Atypia Often present Rare Treatment:
Typically, D&C is performed to initially remove molar tissue. If a molar pregnancy is suspected from the pathological results, HCG levels will be followed until they are undetectable. If HCG fails to decline, methotrexate may also be used to treat the invasive mole. If there is suspicion of a molar pregnancy, the pathology report may provide a comment that biochemical follow-up is recommended.
-
Question 2 of 2
2. Question
HPI: 34 year old G3P4 female with no menses for two years.
Service: Family/Community Medicine
Gross: Received are multiple fragments of scanty red-brown soft tissue (2.0 cm in aggregate).Images:

What is your diagnosis?
Correct
Diagnosis: Placental site nodule with scant strips of inactive endometrium.
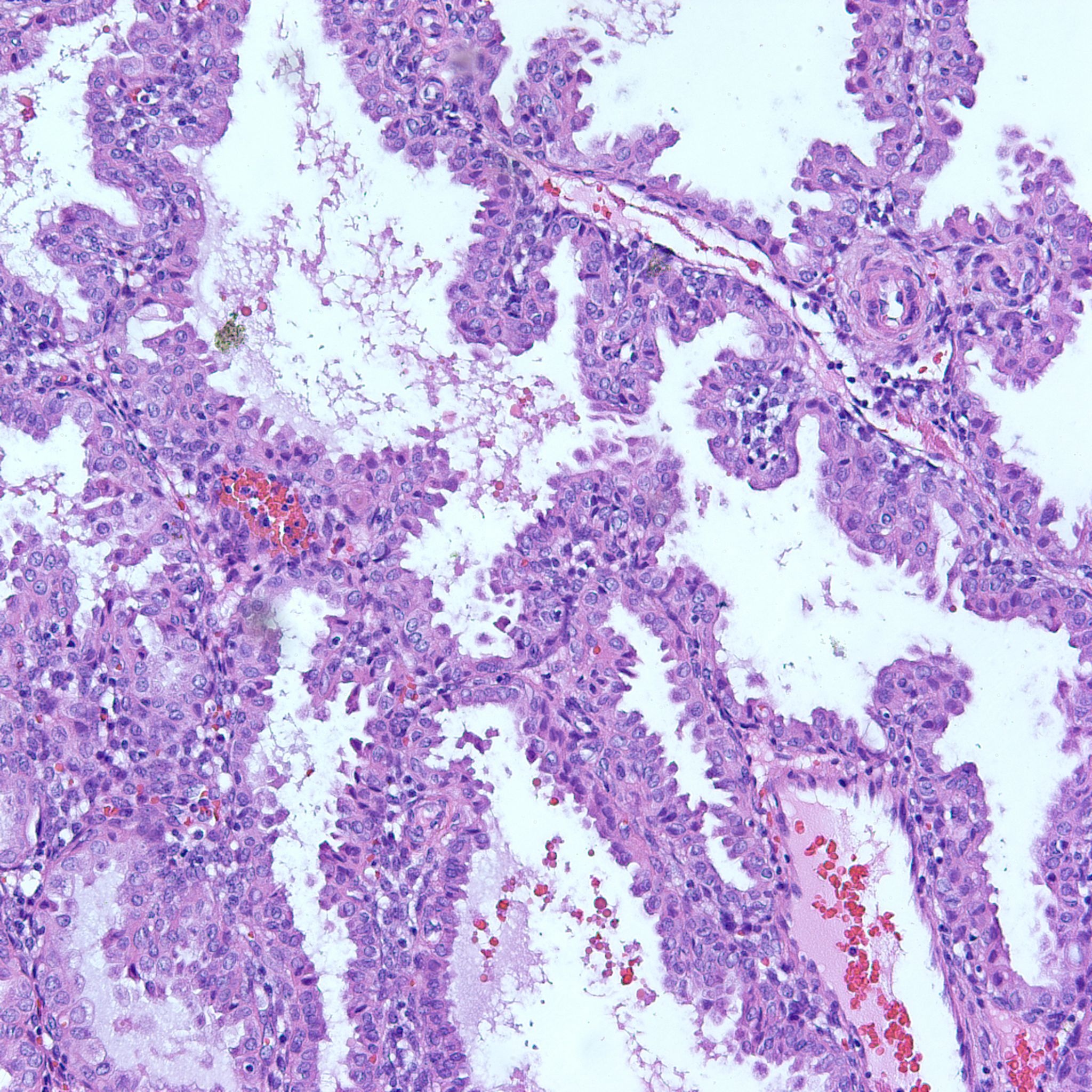
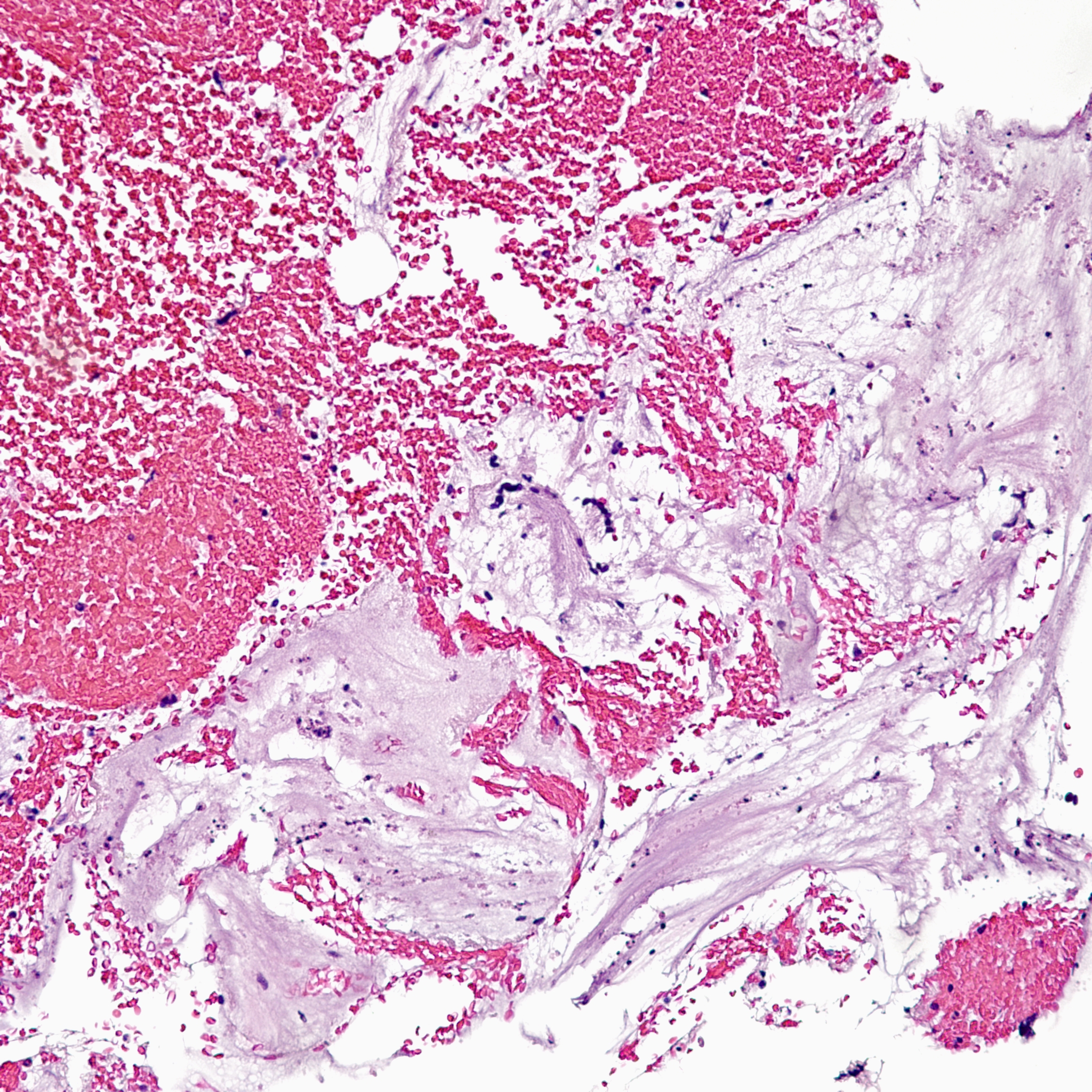
The biopsy contains rare areas like this with scan strips of surface tubal and lower uterine segment epithelium, but without any real appreciable glandular tissue.
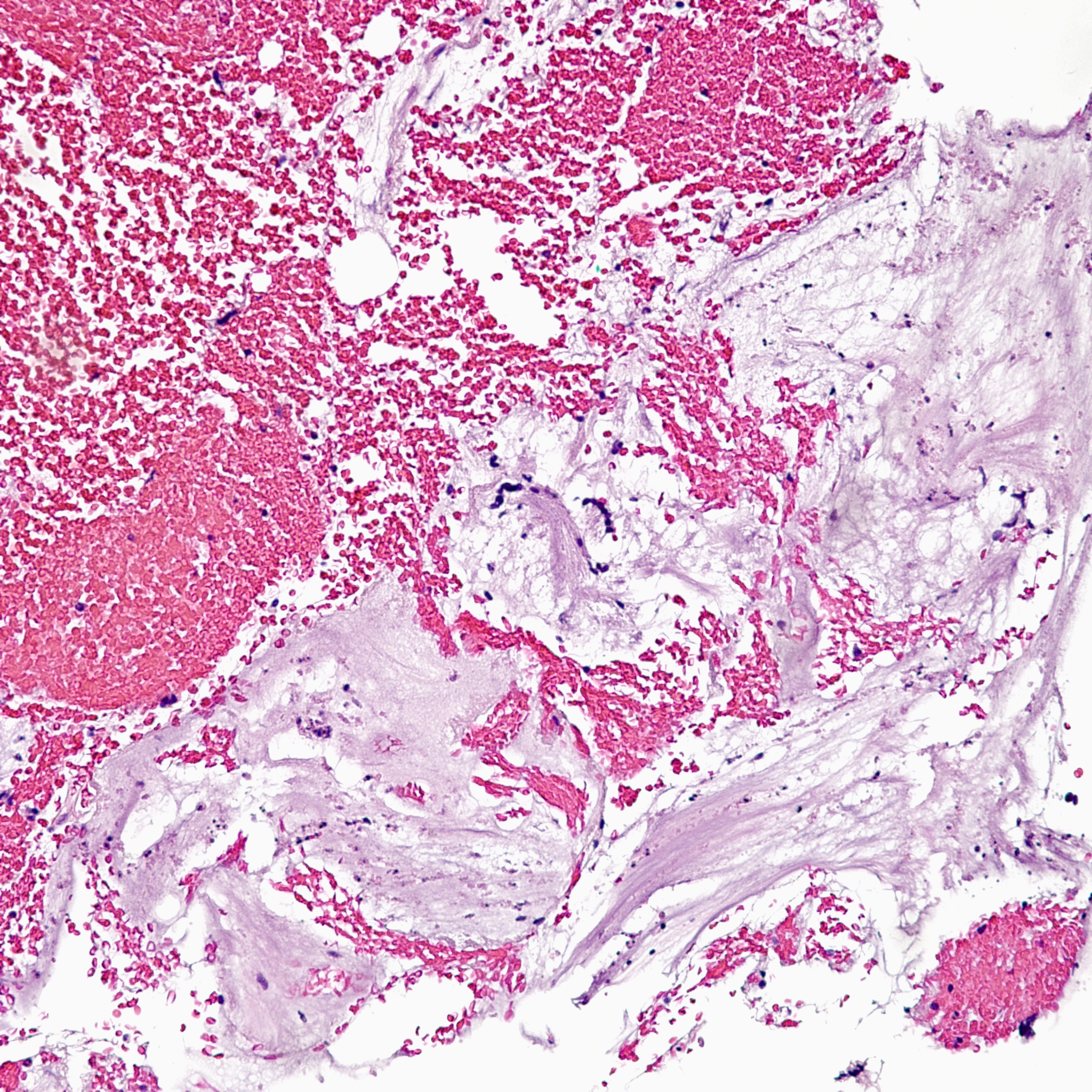
Another major component of the biopsy is blood and wispy grey-pink strands of mucous.
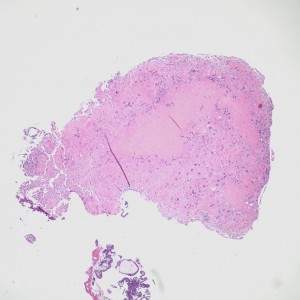
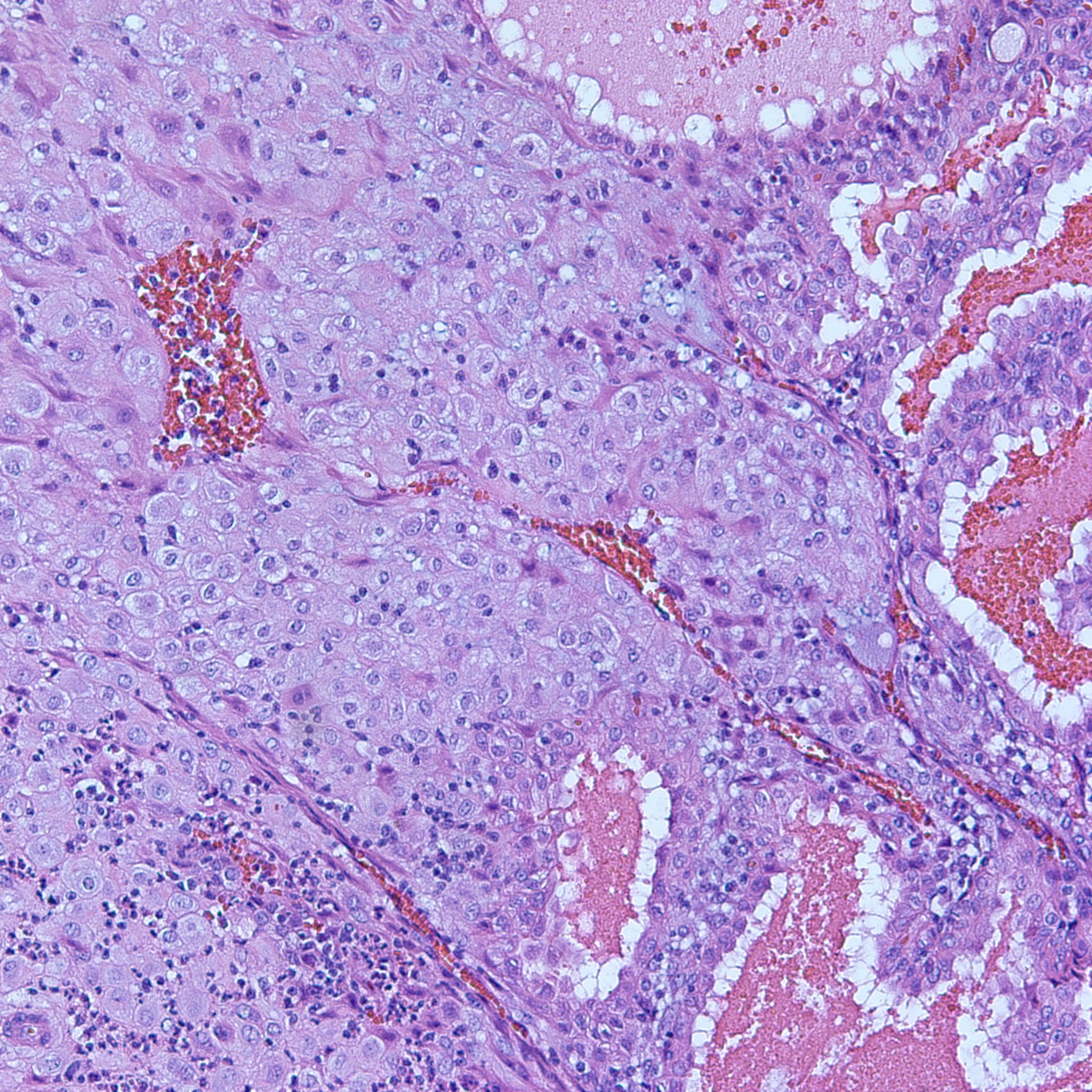
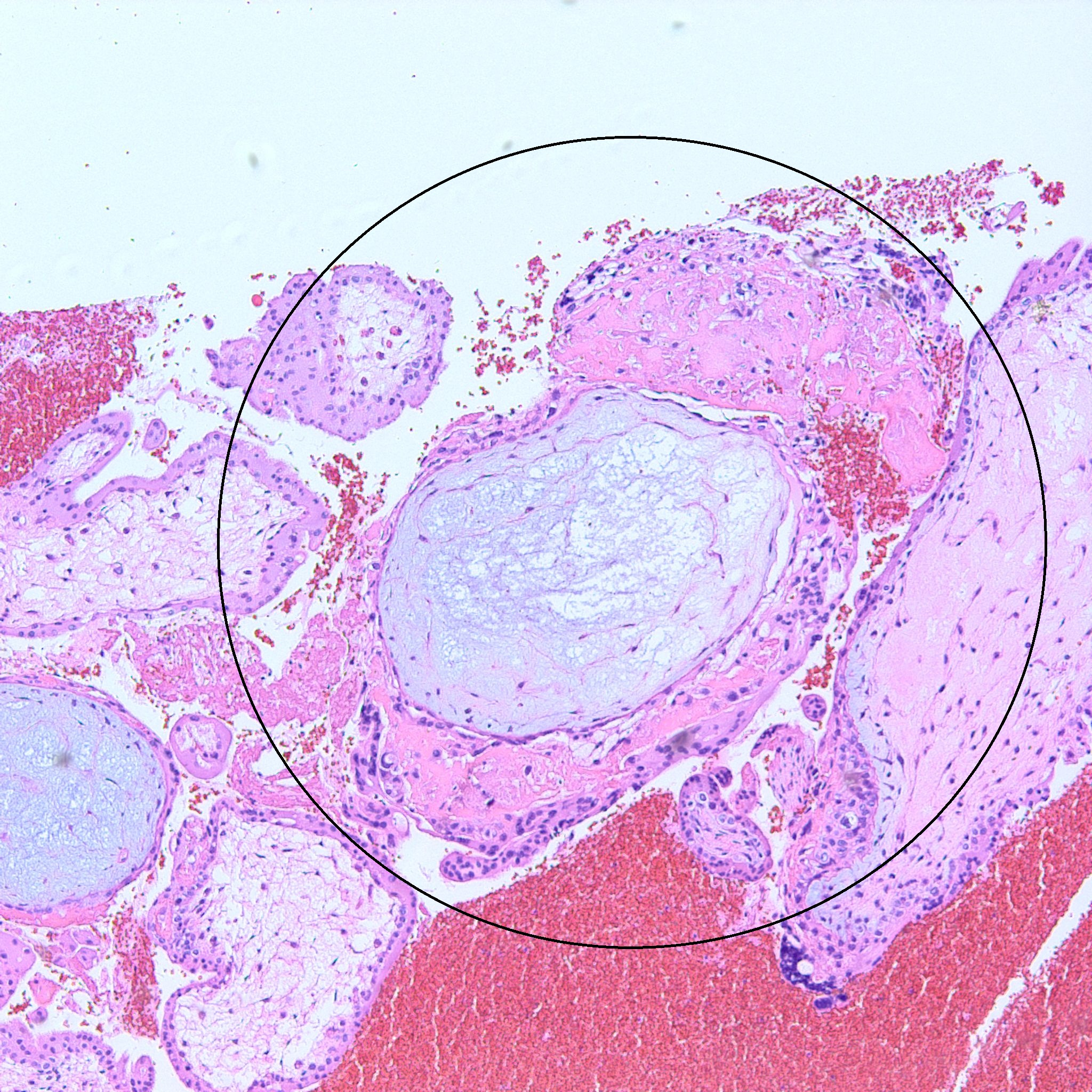
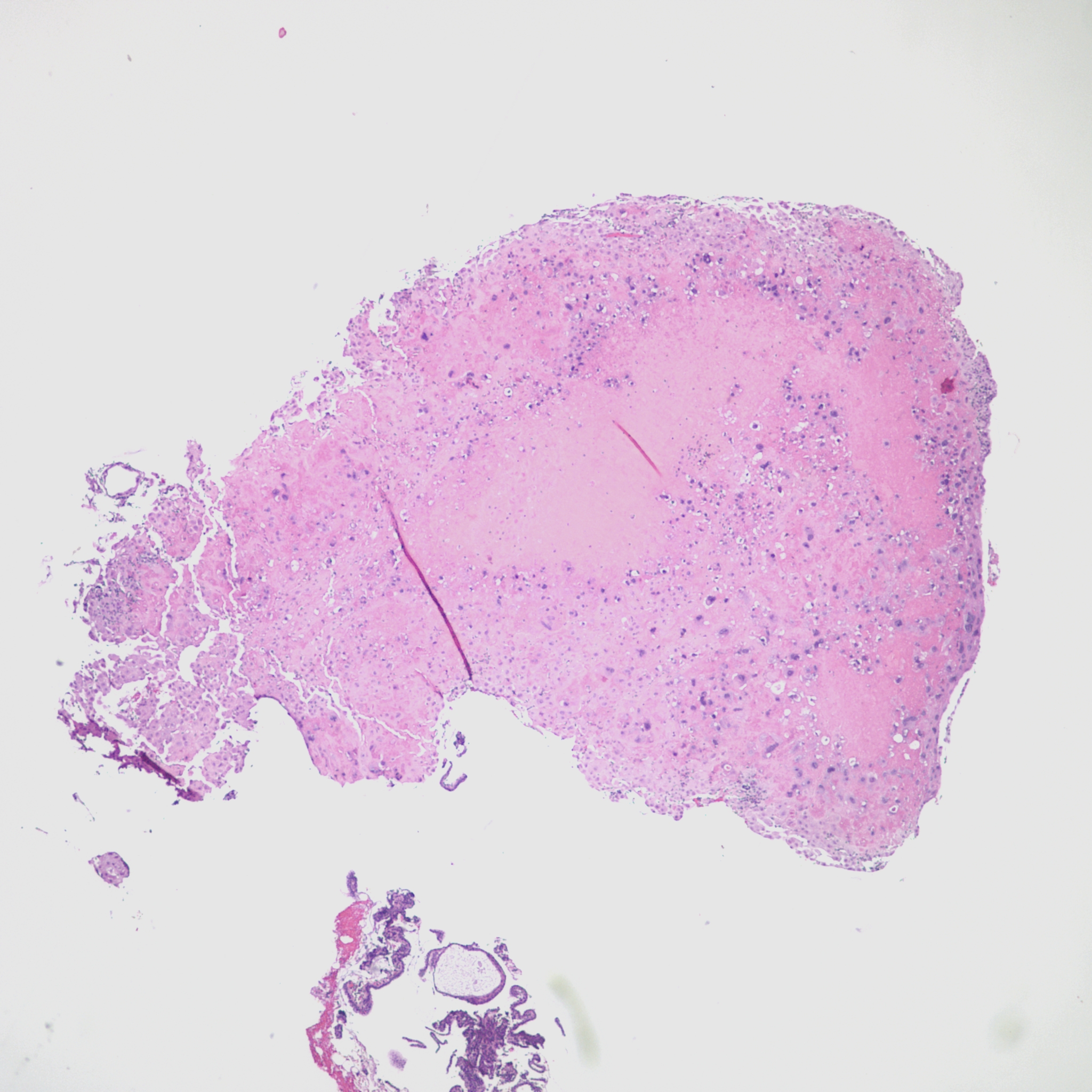
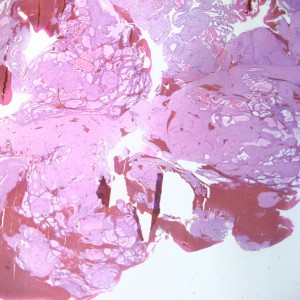
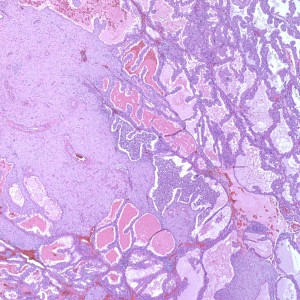
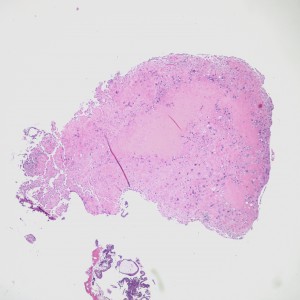
However, in one field we see a well-circumscribed nodule that, on low power, is very pink and glassy appearing, with large cells admixed.
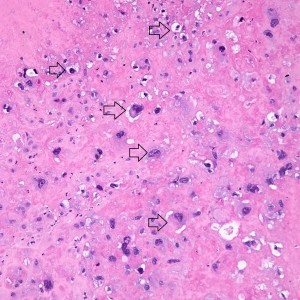
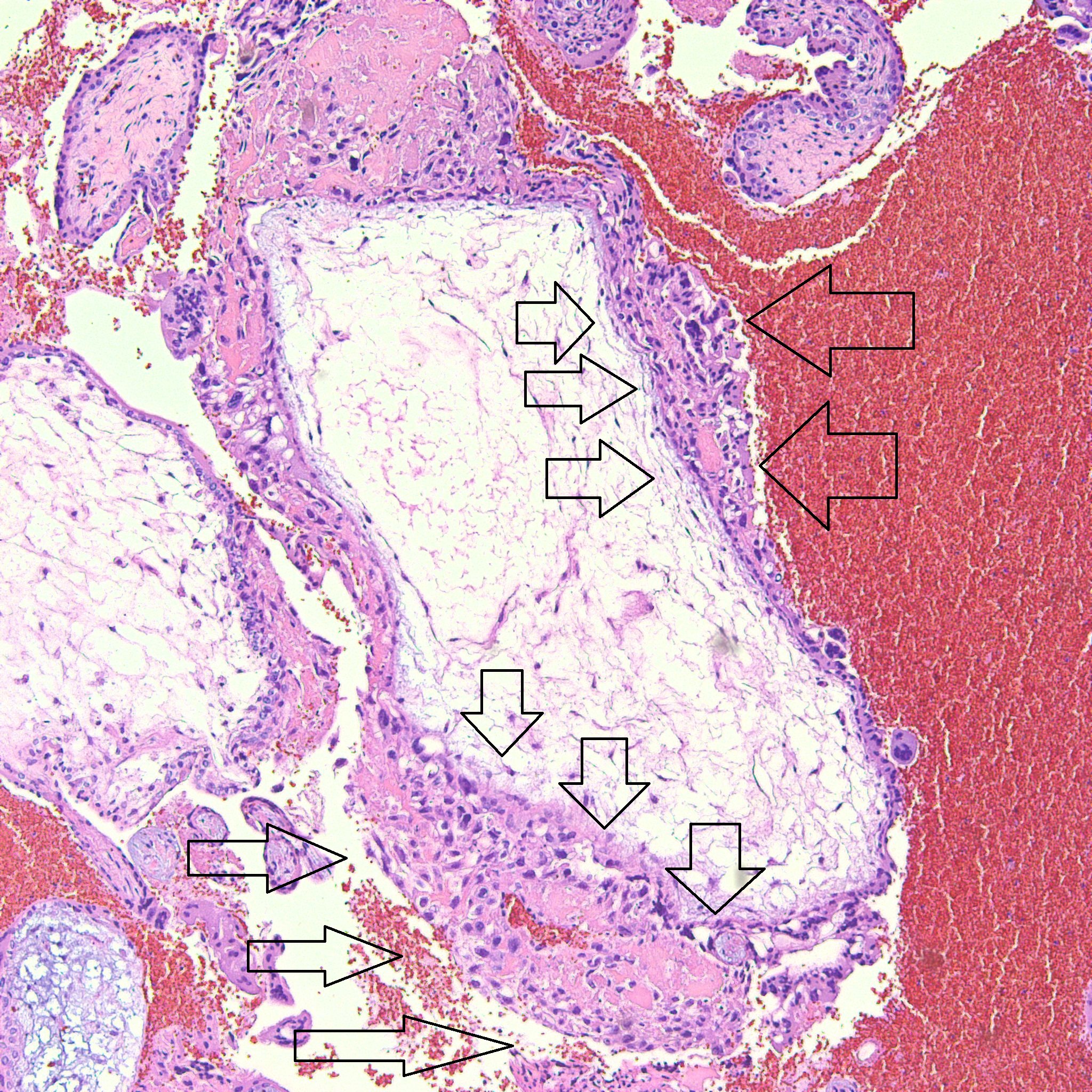
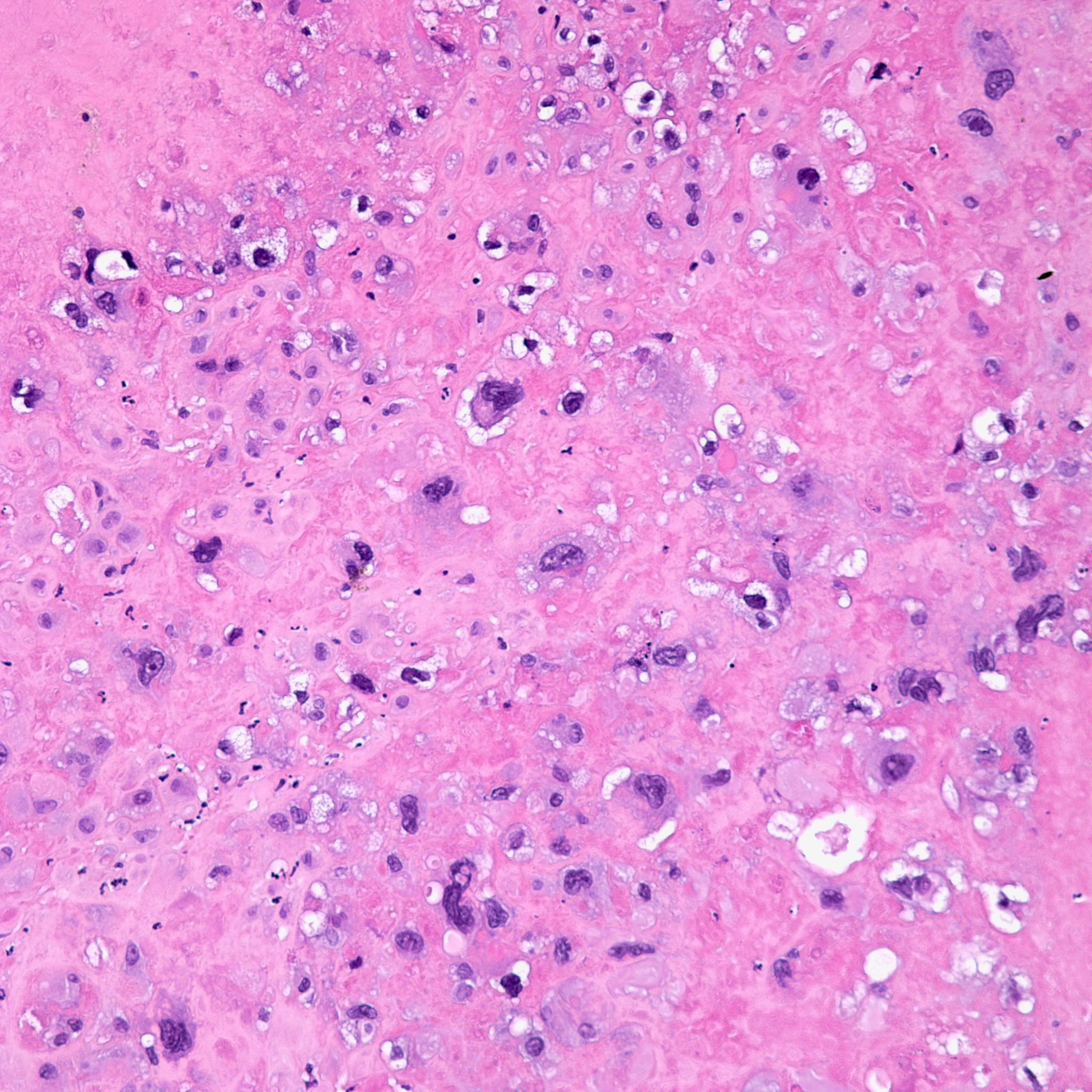
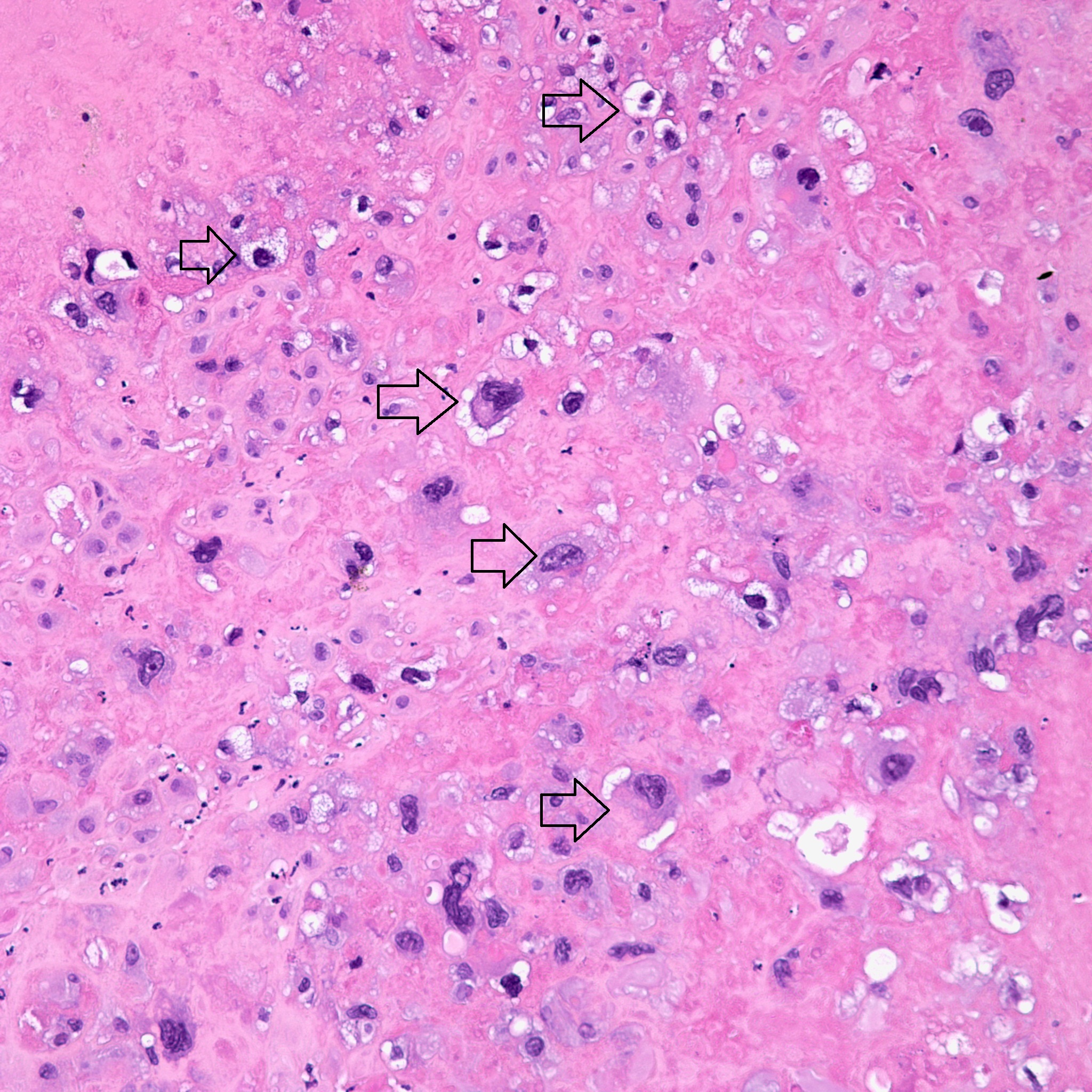
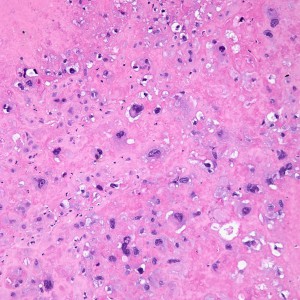
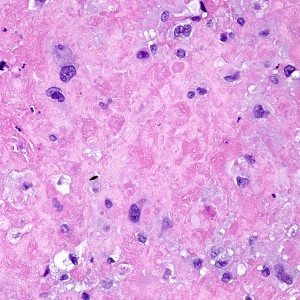
On higher power, we can see that this nodule is mostly composed of this pink amorphous material with interspersed large, round cells with abundant eosinophilic and sometimes clear cytoplasm (arrows). There are essentially no mitoses and atypia is not very prominent.
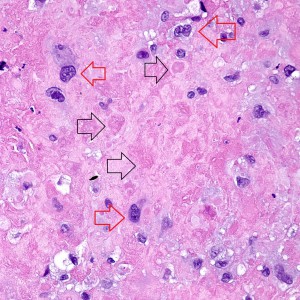
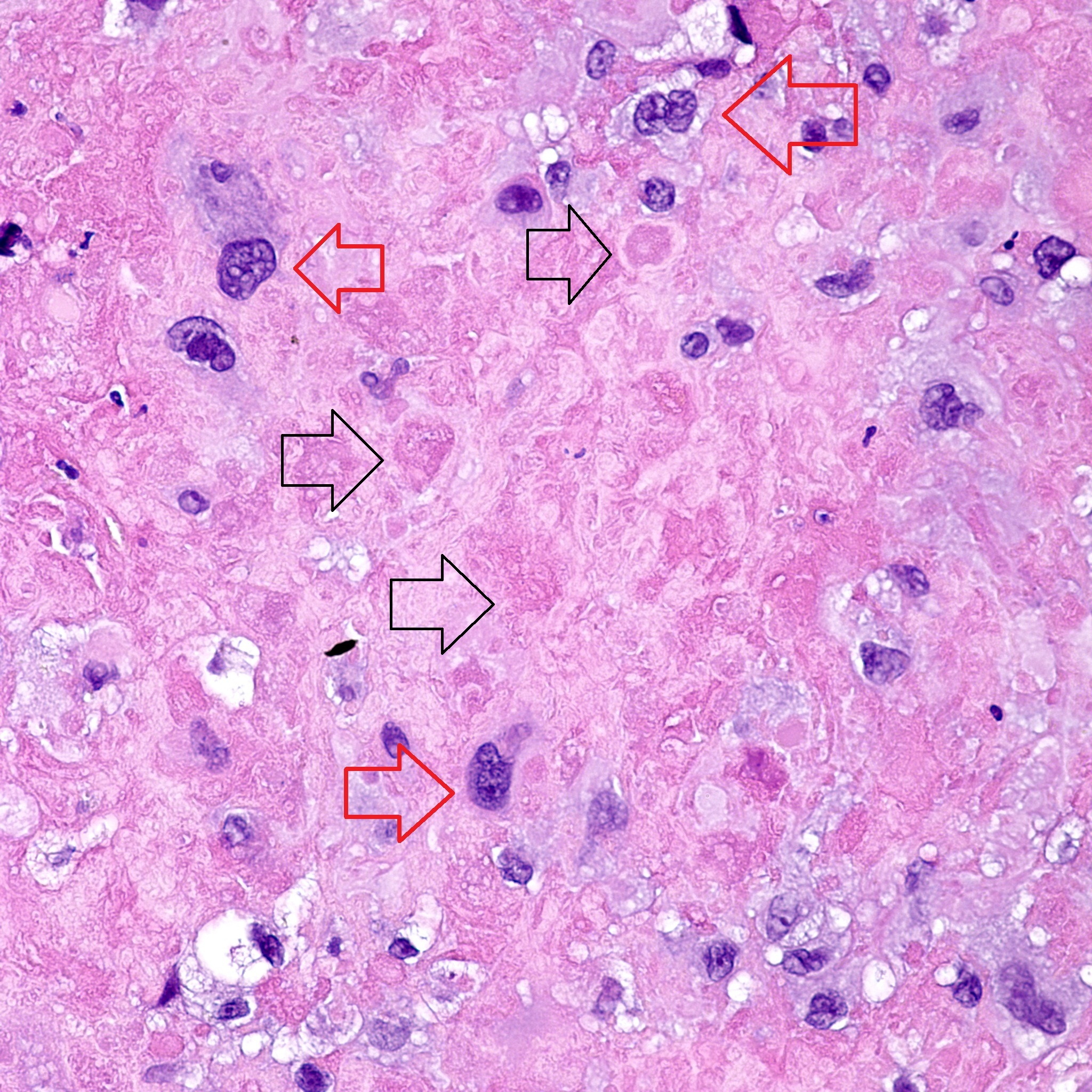
On higher power of the acellular areas we can see vague outlines of the cells that may have been there and have now degenerated into this hyalinized stroma (black arrows). The cells that remain are large, round to oval, with dense eosinophilic to clear cytoplasm (red arrows).
Case Discussion:
Trophoblastic cells are fetal in origin. They form the epithelial component of the placenta. Trophoblasts compose 2 of the 3 components of products of conception. Cytotrophoblasts and Intermediate trophoblasts line villi to form one component. Intermediate trophoblasts (also known as extravillous trophoblasts) form another component, and lastly, fetal tissues form the last component of the products of conception. Syncytiotrophoblasts (ST) and intermediate trophoblasts (IT) are derived from cytotrophoblasts (CT). CT cells are found on the surface of mesenchymal villi. In early pregnancy, IT cells bud off from these CT cells into the surrounding decidua at the implantation site, infiltrating the maternal tissues. Not only are IT cells present at the implantation site, but these IT cells can be seen also on the villi themselves and IT cells also form the chorion laeve within the chorionic layer of the fetal membranes.
Suffice to say:
CT and ST cells: grow in a dimorphic pattern in intimate association with chorionic villi
IT cells: bud off from CT cells to form the implantation site, the chorionic laeve, and may also be found on villi
Morphologically and immunophenotypically, these IT cells exhibit differences:
Villous IT Implantation Site IT Chorionic-Type IT Morphology Polyhedral; abundant, eosinophilic to clear cytoplasm; prominent cell borders Pleomorphic and large, abundant eosinophilic cytoplasm; occasional multinucleated cells Round to polyhedral, regular abundant to clear cytoplasm Cytokeratin ++++ ++++ ++++ Ki-67 90% 0 3-10% PLAP/EMA – – ++ Now, placental site nodule is a small (most often microscopic), well-circumscribed, nodule composed of IT cells that have morphologic and immunophenotypical resemblance to chorionic type IT cells. Hyalinization is a fancy type of degeneration- essentially hyalinization means the tissues impart a homogenous pink “glassy” appearance from degeneration.
After fertilization and implantation, any number of things may occur: abortion, curettage, c-section, etc. In some instances, not all of this implanted material is shed or removed, and it persists in the uterus in the form of degenerative placental site nodules. They have the capability for persisting for many, many, years after pregnancy.
These lesions are entirely benign, but may be associated with abnormal uterine bleeding. In our own case, this nodule was more likely incidental, as the chief complaint was one of amenorrhea.
It is important to differentiate these from two different diagnoses: exaggerated placental site, and placental site trophoblastic tumor (PSTT). PSTT is malignant, and EPS is often found in associated with complete mole(which has its own risks).
Placental site nodule is aptly named- it is nodular and well circumscribed, small, with hyalinization and patchy infiltrative IT cells.
Exaggerated placental site-Essentially, this is the implantation site of a complete hydatiform mole- in comparison to the normal implantation site, invasive trophoblasts appear increased. Moreover these lesions are not circumscribed and do not really exhibit hyaline change. The exaggerated placental site is seen in association with chorionic villi.
PSTT- PSTT will most often form an infiltrative tumor mass (not circumscribed) and is not associated with chorionic villi.
Incorrect
Diagnosis: Placental site nodule with scant strips of inactive endometrium.
The biopsy contains rare areas like this with scan strips of surface tubal and lower uterine segment epithelium, but without any real appreciable glandular tissue.
Another major component of the biopsy is blood and wispy grey-pink strands of mucous.
However, in one field we see a well-circumscribed nodule that, on low power, is very pink and glassy appearing, with large cells admixed.
On higher power, we can see that this nodule is mostly composed of this pink amorphous material with interspersed large, round cells with abundant eosinophilic and sometimes clear cytoplasm (arrows). There are essentially no mitoses and atypia is not very prominent.
On higher power of the acellular areas we can see vague outlines of the cells that may have been there and have now degenerated into this hyalinized stroma (black arrows). The cells that remain are large, round to oval, with dense eosinophilic to clear cytoplasm (red arrows).
Case Discussion:
Trophoblastic cells are fetal in origin. They form the epithelial component of the placenta. Trophoblasts compose 2 of the 3 components of products of conception. Cytotrophoblasts and Intermediate trophoblasts line villi to form one component. Intermediate trophoblasts (also known as extravillous trophoblasts) form another component, and lastly, fetal tissues form the last component of the products of conception. Syncytiotrophoblasts (ST) and intermediate trophoblasts (IT) are derived from cytotrophoblasts (CT). CT cells are found on the surface of mesenchymal villi. In early pregnancy, IT cells bud off from these CT cells into the surrounding decidua at the implantation site, infiltrating the maternal tissues. Not only are IT cells present at the implantation site, but these IT cells can be seen also on the villi themselves and IT cells also form the chorion laeve within the chorionic layer of the fetal membranes.
Suffice to say:
CT and ST cells: grow in a dimorphic pattern in intimate association with chorionic villi
IT cells: bud off from CT cells to form the implantation site, the chorionic laeve, and may also be found on villi
Morphologically and immunophenotypically, these IT cells exhibit differences:
Villous IT Implantation Site IT Chorionic-Type IT Morphology Polyhedral; abundant, eosinophilic to clear cytoplasm; prominent cell borders Pleomorphic and large, abundant eosinophilic cytoplasm; occasional multinucleated cells Round to polyhedral, regular abundant to clear cytoplasm Cytokeratin ++++ ++++ ++++ Ki-67 90% 0 3-10% PLAP/EMA – – ++ Now, placental site nodule is a small (most often microscopic), well-circumscribed, nodule composed of IT cells that have morphologic and immunophenotypical resemblance to chorionic type IT cells. Hyalinization is a fancy type of degeneration- essentially hyalinization means the tissues impart a homogenous pink “glassy” appearance from degeneration.
After fertilization and implantation, any number of things may occur: abortion, curettage, c-section, etc. In some instances, not all of this implanted material is shed or removed, and it persists in the uterus in the form of degenerative placental site nodules. They have the capability for persisting for many, many, years after pregnancy.
These lesions are entirely benign, but may be associated with abnormal uterine bleeding. In our own case, this nodule was more likely incidental, as the chief complaint was one of amenorrhea.
It is important to differentiate these from two different diagnoses: exaggerated placental site, and placental site trophoblastic tumor (PSTT). PSTT is malignant, and EPS is often found in associated with complete mole(which has its own risks).
Placental site nodule is aptly named- it is nodular and well circumscribed, small, with hyalinization and patchy infiltrative IT cells.
Exaggerated placental site-Essentially, this is the implantation site of a complete hydatiform mole- in comparison to the normal implantation site, invasive trophoblasts appear increased. Moreover these lesions are not circumscribed and do not really exhibit hyaline change. The exaggerated placental site is seen in association with chorionic villi.
PSTT- PSTT will most often form an infiltrative tumor mass (not circumscribed) and is not associated with chorionic villi.